A medical worker checks his protective clothing at an MSF facility in Kailahun, Sierra Leone. (Pic: AFP)
For the first time in more than a year, no one in either Sierra Leone or Liberia is being treated for Ebola, raising hopes that after more than 11 000 deaths and 28 000 infections throughout West Africa, the epidemic could finally be winding down.
But 18 months after the World Health Organisation (WHO) formally announced the beginning of the Ebola outbreak in March 2014, the last thing the region needs is another false dawn. Three months ago, Liberia was declared free of the virus only for new cases to emerge.
Although there are just three known cases left in the region and just 629 potential contacts still under observation, the epidemic isn’t yet over.
Here is where things stand:
Guinea
Cases: 3,792
Deaths: 2,527
Guinea is where the outbreak started in December 2013 with the death of a two-year-old boy. Now, 20 months on, much of the country is Ebola-free, including the southeastern forest region where the index case originated. But there remain a few pockets of resistance, particularly in and around the capital Conakry, where the only three current cases in the entire region were recorded during the week ending 23 August. Approximately 600 people are still under observation in Guinea and WHO warns that “there remains a significant risk of further transmission,” particularly because one of the positive cases – a taxi driver who was not previously on any contact lists – could have spread the virus to his passengers. Guinea is also the site of the first health worker infection in more than one month.
Liberia
Cases: 10 672
Deaths: 4 808
Last month, Liberia began a 42-day countdown to being Ebola-free, but not for the first time. The outbreak was previously declared over in the country on 9 May. But on 30 June, the Ministry of Health announced that a teenaged boy had tested positive in a small town on the outskirts of Monrovia. Over the next two weeks, five more cases were confirmed. The source of the second outbreak is still unknown, but Ebola response teams were able to quickly contain the flare-up. The last patient was discharged on 23 July and all potential contacts have since passed the 21-day incubation period. Liberia could once again be declared Ebola-free on 3 September.
Sierra Leone
Cases: 13 541
Deaths: 3 952
Sierra Leone has now gone two consecutive weeks without any new cases being reported. The last patients were sent home as survivors on 24 August. Just 29 contacts are still under a 21-day surveillance period, which is set to end on Saturday. If no new cases surface, Sierra Leone will be declared free of Ebola on 5 October.
A volunteer in protective suit in the capital Freetown. (Pic: AFP)
For the last 13 years, Sierra Leone has seen a dramatic decrease in its maternal mortality rate, due in large part to the introduction of free health care for pregnant women. One of the most devastating and yet rarely acknowledged impacts of the Ebola epidemic is that it threatens to undo all this good work.
It’s not just the loss of more than 220 health workers, including many midwives, to the virus, with little training or wiggle-room in the fragile health system to replace those skills. It’s also the lingering fear of hospitals and doctors among the local population, which remains traumatised by an outbreak that has claimed almost 4 000 lives and still sees new infections each week, albeit small numbers.
A World Bank report in July – Healthcare Worker Mortality and the Legacy of the Ebola Epidemic – estimated that Sierra Leone’s maternity mortality rate could increase because of the current crisis by 74 percent, to levels not seen since the end of the civil war in 2002.
“During the Ebola outbreak, there were many challenges that we encountered that led to many pregnant women not coming to the hospital and this may have led to the [recent] increase in death rates [among pregnant women],” A.P. Koroma, medical superintendent at the PCMH (Cottage) Hospital in Freetown, told IRIN.
The hospital has lost 85 mothers since the outbreak was first reported in May 2014, which Koroma said is “definitely a sharp increase compared to previous years.”
“People were, and are [still], afraid,” he added.
Before Ebola came, an average of 10 700 women each year gave birth at Cottage Hospital. Since the outbreak, this number has dropped to 6 723.
The most recent maternal mortality rate is not yet available at the national level, but given the hospital attendance records and the risks of at-home childbirth in Sierra Leone, it is expected to rise.
“During the Ebola outbreak, people had the impression that when they come to the hospital, they may be infected,” Koroma explained. “For those coming to the hospital, we did our best… but some of them came to the hospital late because they were told that if you have bleeding, which is one of the symptoms of Ebola, no nurse or doctor will want to touch a patient until an Ebola test is done, which can take up to three days.”
Others, who did come, died while waiting for the Ebola test results.
The hospital now has access to a rapid diagnostic test, which can give results in less than three hours.
Despite this, and better safety measures generally, many hospital staff are still afraid to tend to pregnant women, given the fact that childbirth puts them in direct contact with bodily fluids.
“When we started hearing of our colleagues dying, everybody was afraid and nobody wanted to even touch a patient,” Koroma explained.
But not all women are staying away.
“Some of my friends said that if I came to the hospital I would get Ebola… so I became afraid,” said 22-year-old Mary Conteh, from Freetown, who gave birth earlier this month. “But later I decided to come to Cottage Hospital…. I thank God I had a safe delivery.”
Shortage of health workers
Sierra Leone lost an estimated seven percent of its nurses and midwives to Ebola, according to the World Bank report – a devastating loss for a country that had just over 1 000 to begin with.
“This is just a terrible shock to an already weak healthcare system,” said David Evans, Senior Economist at the World Bank Group. “And if one were to put this [loss of health care workers] into actual numbers, that’s an additional 1,850 women dying per year [in Sierra Leone] just as a result that we’ve lost health care workers due to the Ebola epidemic.”
If Sierra Leone is to prevent its maternal mortality rate rising further, experts say more investment is drastically needed to plug the gap in maternal healthcare.
“In terms of response, it’s not rocket science,” Evans said. “These countries and the international communities supporting them need to hire more health workers and provide resources so they are well paid and want to be in Sierra Leone working there. And, as the Ebola epidemic wanes, as it continues, making sure they have protective equipment.”
In the short-term, to avoid a further increase in maternal mortality, Evans suggested a “stop-gap measure” of employing foreign healthcare workers and birth attendants, allowing local capacity to be built up over the longer term.
Women in Sierra Leone say they are praying for just that.
“All I want is to have a healthy baby,” said 25-year-old Frances Tucker, who is five months pregnant. “I don’t want to have problems like other pregnant women have had by staying at home, afraid of coming to the hospital… putting you and your baby’s life at risk.”
Bystanders watch as a suspected Ebola victim waits to be transported from Devils Hole North, west of Freetown. (Pic: Reuters)
Brian Lomax (26) sleeps on a pile of bones – the remains of cremated Ebola victims whose relatives may never get the chance to collect.
He was hounded out of his community by neighbours who feared his work at the Margibi crematorium in Boys Town, Lower Margibi county, was helping to spread the disease rather than contain it. This is the only place he has left to go.
Lomax is just one of many Liberians whose lives have been altered by the cremations at Margibi, which came to an end in December after a burial site was found for new victims.
For authorities and health workers, who believe they are now beating back the virus, the cremations – an alien and unwelcome practice in Liberia – were a successful measure that helped contain the disease.
“Cremation is not our culture. It was due to necessity that we had to cremate people, but it worked very well,” said Tolbert Nyensuwah, head of the government’s Ebola task force.
However, over the past four months, waves of protests have taken place against it. Those who worked at the facility are left facing stigma, and the relatives of those who were cremated have no graves for their loved ones.
Liberia was the country hardest hit by the Ebola outbreak, which has now claimed over 8 500 lives. In the midst of the crisis, disposing of the bodies of victims quickly and safely had been, and remains, paramount, as the bodily fluids from the corpses can still transmit the virus.
By August last year, Liberia’s government was struggling to keep up with the rising death toll. Underpaid, under-equipped and overworked burial workers couldn’t cope. When teams clad in space-man like protective suits came to collect victims, terrified residents often chased them out.
‘Nights of terror’ When members of Margibi county’s Indian community, which ran the Margibi crematorium 50 miles from the capital, offered to help, it seemed like an obvious solution. A group of Liberians were quickly taught how to carry out the Indian cremation method to dispose of the bodies.
Sometimes up to a hundred bodies were burned at once. Members of the community living nearby reported huge explosions as it burned with smoke rising through the air. Disturbed by the process, they called it ‘nights of terror’.
The burial process and honouring deceased relatives is an important tradition in Liberia, and often involves touching the body of the deceased. On decoration days, crowds visit cemeteries to clean and decorate the graves of relatives. The cremations, which were often rushed and en masse, left many relatives alienated, and often unable to locate and identify the remains of their loved ones.
Lomax, a student who had never worked in a crematorium before, was one of those who volunteered to work at the crematorium. “[We] opted for it because we had to do a service to the country because no one wanted to do such a work,” Lomax said.
“When they [the government] got here, they put us together and told us that this issue was an emergency issue, so we did not discuss anything with them,” he said. “All of a sudden they started the method that the Indian people taught them. They started training us on the method to carry out the cremation.”
The process of cremation burns corpses, but the bones then have to be ground to a powder afterwards – a stage that was neglected in the Margibi crematorium.
“All these containers are filled with human bones and because we have nowhere to go, we sleep with the bones [inside this] fence,” Lomax said, pointing to a row of steel drums which he and his colleagues were placing wooden planks over to form makeshift beds every night.
But promises that the ashes of Ebola victims would be handled respectfully and returned to family members quickly unraveled. The overwhelmed workers at Margibi didn’t know what to do. Some days, dozens of corpses arrived. Hundreds are thought to have been cremated at the site between August and December.
“This is the largest altar where we burned 145 bodies. The ashes were too much, and we had nowhere to put them. [Back] then we had no knowledge of bringing in drums,” Lomax explained, referring to the steel drums brought in by the government when they decided to preserve the ashes.
“So we just wasted [dumped] it in these holes. Later they decided that we use the drums,” he said. For those whose bones and ashes could not make it into the zinc containers, their bones are all dumped in a pit resembling a mass grave.
“This is how people who died from this deadly disease were treated here,” said Lomax.
Bones lie waiting to be claimed The Boys Town community called for all cremations to stop, and eventually a new burial ground was found on Disco Hill, also in Margibi County, where Ebola victims will be interred from now on.
Bone fragments are seen in a barrel of the cremated remains of Ebola virus victims in Boys Town on January 9 2015. (Pic: Reuters)
The bones now sit in silent rows, unmarked for any relatives who might want to claim them back. The only clue to the identity of those who remains are stored inside are the dates scrawled on the side of each container.
Lomax has been outcast for his work at Margibi, believed to be the country’s only crematorium for Ebola victims.
“My father has his house right behind here but he told the children I shouldn’t go there because I am working here and burning Ebola bodies. He said he does not want me to carry the virus to his house,” he said quietly.
Just over a month ago, their bosses stopped coming to work and he worries about money. He and his colleagues fear they may never reintegrate into society.
“For the past three weeks we have not seen our bosses. After all that we have done, at least we should have been settled [paid].”
Tibelrosa Tarponweh, a local resident, called for counselling services to “ be provided to members of the community, including a select few that were hired without proper guidance to perform such an abnormal task.” He said the lack of training for Lomax and his colleagues had led to a “sloppy and harmful” process.
He called for the government “to secure and preserve the now-defunct crematorium for use as a shrine in memory of our fallen compatriots.”
Wade Williams and Monica Mark for the Guardian Africa Network
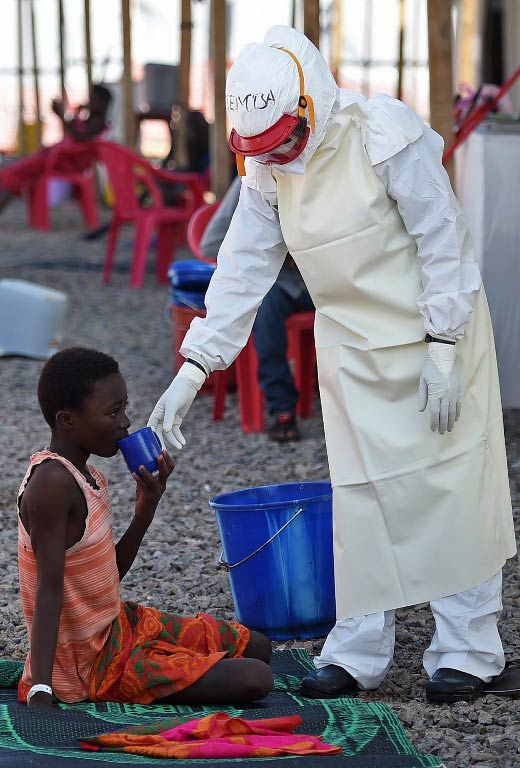
A health worker gives a drink to a young Ebola patient at the Kenama treatment centre run by the Red Cross Society. (Pic: AFP)
Junior doctors at Sierra Leone’s main hospital went on strike on Monday in protest over inadequate equipment to fight the Ebola epidemic ravaging the impoverished nation.
The action at Freetown’s Connaught Hospital follows the deaths of three doctors in two days, with new figures showing Sierra Leone has overtaken Liberia as the country with the most infections.
“We have decided to withhold our services until proper and more conducive atmosphere is created for us to continue our work,” the Junior Doctors Association said in statement.
The association did not say how many doctors were joining the action, but patients were reporting significant disruptions as senior consultants headed to the wards to cover their work.
One junior told AFP she and her colleagues were “depressed” and “losing courage to turn up for work” because of the lack of equipment.
“We are also worried over the deaths of our colleagues… which is very disheartening,” she said.
The doctors say they don’t have enough respiratory machines and vital signs monitors, and that intensive care facilities are lacking in an Italian-built treatment centre in the west of the city to which some them are due to be sent.
A source at the Junior Doctors Association said the union would meet on Tuesday to decide whether to continue the action.
The World Health Organisation published new figures on Monday showing that Sierra Leone was registering the most cases in west Africa, for the first time, with 7 798 cases compared with Liberia’s 7 719.
Sierra Leone has recorded around 1 742 Ebola deaths this year and has registered a worrying surge recently of cases in its western area, including the capital.
Ten Sierra Leonean doctors have died after contracting Ebola.
Aiah Solomon Konoyima’s death late on Saturday at an Ebola treatment unit in Hastings, near the capital Freetown, came just a day after two of his colleagues were killed by the virus.
Even before the Ebola epidemic spread from Guinea in May, Sierra Leone, one of the world’s poorest countries, was still struggling to rebuild its health services after a decade-long civil war in the 1990s.
In 2010 the nation was estimated to have around one doctor for every 50 000 people – or roughly 120 doctors for the entire country.
The doctors are among more than 300 healthcare workers to have died treating patients infected in the deadly outbreak, which appears to be stabilising in Guinea and Liberia but is still spreading at an alarming rate in Sierra Leone.
The virus is spread through contact with bodily fluids, meaning healthcare workers are particularly at risk, and more than 100 have lost their lives in Sierra Leone.
The outbreak has left more than 6 300 people dead worldwide since December 2013, nearly all in Sierra Leone, Guinea and Liberia.
A volunteer in protective suit looks on after spraying disinfectant outside a home in Waterloo, 30km from Freetown. (Pic: AFP)
Watching with horror as the Ebola crisis ravages their country, Sierra Leoneans in London are mobilising to help their compatriots fight the deadly virus back home.
Health workers are taking leave from their jobs in the state-run National Health Service (NHS) to volunteer in Sierra Leone, where at least 1 200 people have died so far.
Others are raising funds for medical supplies, protective clothing and even hot meals for those affected – anything that makes a difference.
“I see it as a call of duty – I need to go down and help my people,” said Ajan Fofanah, a 46-year-old trained paediatric nurse who has applied to spend eight weeks working in Sierra Leone.
He was born in the west African country and moved to Britain aged 27 to further his education. Now he wants to use his skills to help battle the virus that has killed four members of his extended family.
“I’m far away from them and this is what is heart-rending. I need to get closer,” he added.
Fofanah was one of around 80 Sierra Leonean medics who attended an event in London last week to find out more about how they could help.
All were successful professionals keen to put their careers in Britain on hold and even risk being infected with Ebola to help their country.
Mohamed Koker, a 50-year-old emergency doctor who has worked in Britain for 12 years, hoped his knowledge of languages and traditions would help break down barriers with locals.
“I think the urge within me to perform what I call a national duty overrides my fear,” he told AFP.
“Most importantly, I have all the Sierra Leoneans back home who have no medical knowledge and who are sacrificing themselves, who are doing more than I think I am doing here.”
It is not only doctors and nurses who are desperate to help.
The British government is leading the international aid effort in its former colony, but members of the 23 000-strong Sierra Leonean diaspora here want to go further.
Ebola “is the only topic of conversation” among many, said Ade Daramy, chairman of the Sierra Leone Diaspora Ebola Task Force, which is working to help co-ordinate the response.
Food campaign, clothing “When you live overseas and you’ve got family there – that just breaks you,” added Memuna Janneh, a 46-year-old British business consultant who grew up in Sierra Leone.
She started a charity in London to help feed people working on the frontline in Freetown, helped by her husband and relatives who are still living over there.
“LunchBoxGift” provided 2 600 meals to people living rough during the three-day lockdown in September, and now hopes to provide 50 000 more to hospital workers and patients.
“We may not have the cure, we may not have the logistics, we may not have the hospitals, all of those more complicated things that the government is battling to deal with,” she told AFP.
“But we can certainly as ordinary people come together to do food. It was really that simple for me.”
The British-based Sierra Leone War Trust for Children (SLWT) has also raised money to provide protective clothing and non-contact infrared thermometers for health workers and to deliver handwashing stations to rural areas.
In another innovative project, it sent 1 000 plastic raincoats to provide basic protection from Ebola for drivers of the “okada” motorcycles commonly used for transport.
For some, the urge to help is fuelled by a desire to save Sierra Leone from another trauma as serious as the country’s 1990s civil war.
Mayene Sesay (32) saw her mother shot dead in 1999 and lost a foot when a house she was in was set on fire.
She now runs an NGO for young disabled people in Sierra Leone.
Although not a medic, she attended the recruitment event in London to find out what she could do to fight Ebola.
“Whatever happens to me, I’m going to stay strong and help my country because I don’t want (it) to go through something else again,” she said.
“At least I can remember the person who shot my mum but I cannot see Ebola, where it comes from, how it affects my family. It’s like a ghost – you’re gone.”